Welcome to Xi’an Good Doctor Medical Science and Technology Co., Ltd.website !
Internet Drug Information Service Qualification Certificate: (Shaanxi)-Non-Operating -2023-0143


Forwarding: Quality Control Considerations for Intraperitoneal Hyperthermic Chemotherapy: How to Avoid Instability in Perfusion
For peritoneal carcinomatosis or malignant ascites, hyperthermic intraperitoneal chemotherapy (HIPEC) is the standard approach. Of course, some patients undergo cytoreductive surgery (CRS) before HIPEC to reduce tumor burden and even achieve radical resection of organs affected by the tumor for better efficacy. Here, we focus on infusion instability.
2025-04-07
Quality Control Considerations for Intraperitoneal Hyperthermic Chemotherapy:
How to avoid perfusion instability
For peritoneal carcinomatosis or malignant ascites, Hyperthermic intraperitoneal chemotherapy (HIPEC) is already a standard approach. Of course, for better efficacy, some patients will undergo CRS before HIPEC to reduce tumor burden or even achieve radical resection of tumor-involved organs. Here, we focus on perfusion instability.
1. What is perfusion instability?
The goal of HIPEC is to maintain two indicators: 1) Temperature maintenance, no less than 41℃, preferably at 43±0.5℃. Due to the lack of uniformity and inconsistent parameters of hyperthermic perfusion equipment worldwide, internationally, it is generally considered that the temperature should not be lower than 41℃. 2) The flow rate of the perfusion fluid must be around 1100ml/min, but what is the upper limit? Further research is needed.
2. Parameters that may be involved in ensuring perfusion stability include: 1) Equipment performance; 2) Catheter placement; 3) Volume of perfusion fluid. Literature suggests: Calculated according to body surface area and gender, it is generally 2000ml/m² for women and 2500ml/m² for men. However, what this standard corresponds to for the Chinese population still needs further research.
Figure 1. Reference 1,
The authors are a nursing team from Italy.
3. The Italian team conducted a study on the above issues (see the literature in Figure 1), believing that through reasonable management of the drainage tube position, muscle relaxation control, patient body position adjustment, perfusion volume adjustment, and drainage tube flow rate switching, the above problems can be eliminated.
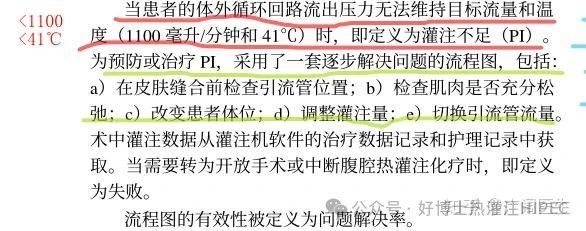
Figure 2. Solutions for insufficient perfusion
While reading these articles, I was also thinking: We need to develop a formula for determining the perfusion volume for the Chinese population, rather than using a uniform volume of 3000 or 4000 ml. We need to consider the actual volume of the peritoneal cavity to ensure a constant flow rate and temperature. Because only with the appropriate peritoneal cavity volume to maintain the flow rate and temperature can the perfusion be kept constant/stable, and the desired effect after injecting chemotherapeutic drugs can be ensured.
To this end, I also consulted domestic HIPEC equipment manufacturers, who believe that the above problems are the shortcomings of the existing hyperthermic perfusion equipment in the domestic market. A hyperthermic perfusion instrument manufacturer in Xi'an believes that they solved the phenomenon of the abdominal cavity temperature not reaching 41 degrees from the beginning, because their hyperthermic perfusion instrument does not have the phenomenon of reflux pressure and flow rate not reaching the target flow rate and temperature. With a catheter diameter of 24-26 Fr, the temperature can basically reach 42 to 42.5 degrees. An important reason is that the temperature of this equipment is adjustable. In addition, a very important point is that this equipment does not rely on abdominal pressure for natural outflow, but uses power to negatively drain the perfusion fluid.
However, relevant technical personnel also admitted that the issue of the volume of peritoneal perfusion is indeed a difficult problem. Different people have different peritoneal cavity volumes. Men, women, and women who have given birth have different peritoneal cavity volumes. Therefore, it is difficult to define it. How to calculate it? A formula is indeed needed. This is a mathematical problem. Perhaps in the future, through interdisciplinary collaboration, we can see how mathematical experts can solve this problem.
4. Finally, I would like to raise another question for everyone to consider: The physical volume of the peritoneal cavity can still be assessed, at least it can be measured, but the volume suitable for hyperthermic perfusion is not necessarily easy to calculate, because the abdominal wall deforms under a certain pressure, and the internal organs (intestinal cavity) also deform. The effective peritoneal cavity perfusion volume needs further research. I consulted the omnipotent AI tool, and we obtained some information, which everyone can take a look at. This is just a starting point!
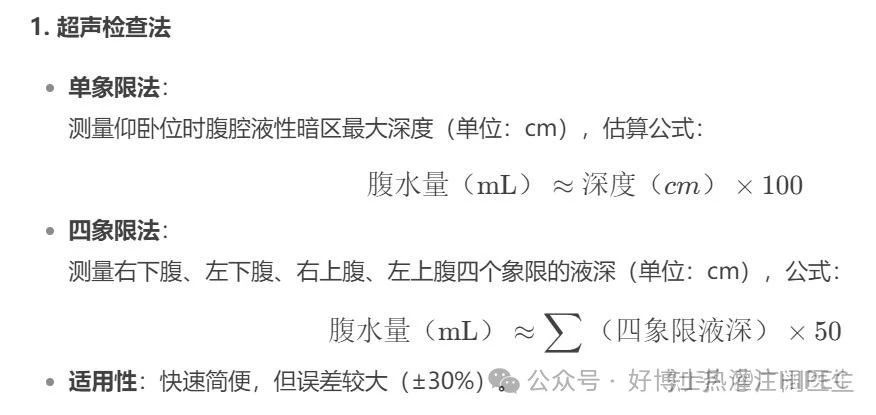
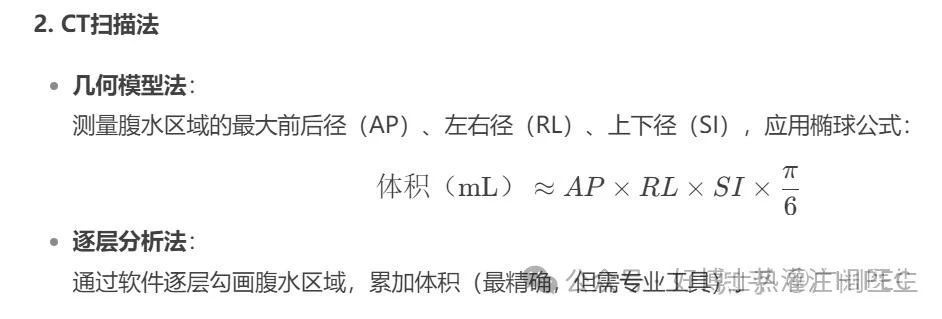
Figure 4. Evaluation using CT
In short, there is no exact method. Perhaps in the future, AI assistance and automatic segmentation algorithms based on CT/MRI can improve the accuracy of the evaluation. Bioelectrical impedance is also a method (experimental technology, estimating the amount of liquid through the difference in electrical signals), which can be used for reference.
(Reprinted from: Malignant Pleural and Peritoneal Effusion CRS+HIPEC Column)
Key words:
Related News

· China Good Doctor ·
· Good friends of human beings ·
Address: Floor 1-2, Left Building No. 1, Huoju Road, East zone of Xi’an High- tech Development District, Xi’an, China
Copyright Xi'an Good Doctor Medical Technology Co., Ltd.
Internet Drug Information Service Qualification Certificate (Shaanxi)-Non-Operating -2023-0143